Congenital heart defects are structural problems in the heart that are present at birth. These conditions affect how the heart develops and functions, impacting blood flow and oxygen circulation throughout the body. Some defects are mild and may not require treatment, while others can be serious and need immediate medical care.
Understanding different types of heart defects, their symptoms, causes, and treatment options helps parents and caregivers take timely action and ensure better outcomes for children.
What Are Congenital Heart Defects
Congenital heart defects refer to abnormalities in the structure of the heart that develop during pregnancy. These may involve the walls of the heart, valves, or blood vessels.
They are among the most common birth conditions and vary widely in severity. Some children may live normal lives with minimal intervention, while others may require surgeries or lifelong monitoring.
Types of Congenital Heart Defects in Children
Congenital heart defects are broadly classified into two categories:
Cyanotic Heart Defects
These defects reduce oxygen levels in the blood, causing a bluish tint to the skin.
- Tetralogy of Fallot
- Transposition of the great arteries
- Tricuspid atresia
- Total anomalous pulmonary venous return
Acyanotic Heart Defects
These defects usually do not affect oxygen levels initially but can still lead to complications.
- Atrial septal defect
- Ventricular septal defect
- Patent ductus arteriosus
- Pulmonary stenosis
- Aortic stenosis
List of Common Congenital Heart Defects
Below is a detailed list of frequently seen heart defects in children:
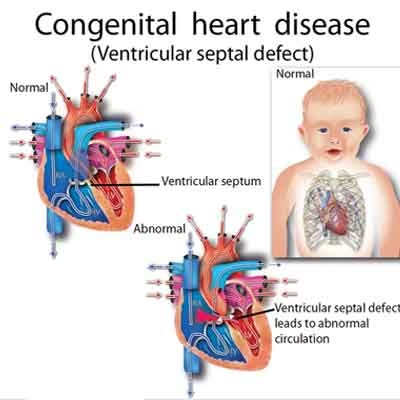
Ventricular Septal Defect
- A hole in the wall separating the lower chambers of the heart
- One of the most common heart defects
- May close on its own in mild cases
Atrial Septal Defect
- A hole between the upper chambers
- Can cause increased blood flow to the lungs
- Often diagnosed later in childhood
Patent Ductus Arteriosus
- A blood vessel that fails to close after birth
- Leads to abnormal blood flow
- More common in premature babies
Tetralogy of Fallot
- A combination of four structural abnormalities
- Causes reduced oxygen levels
- Often requires surgical correction
Pulmonary Stenosis
- Narrowing of the pulmonary valve
- Restricts blood flow to the lungs
Aortic Stenosis
- Narrowing of the aortic valve
- Affects blood flow from the heart to the body
Transposition of the Great Arteries
- Major arteries are reversed
- Requires immediate medical intervention
Coarctation of the Aorta
- Narrowing of the aorta
- Leads to high blood pressure and reduced blood flow
Tricuspid Atresia
- Missing or abnormal tricuspid valve
- Affects blood flow between heart chambers
Most Common CHD and Heart Defect
- Ventricular septal defect is considered the most common congenital heart defect
- Atrial septal defect and patent ductus arteriosus are also frequently seen
- Early diagnosis improves treatment outcomes
Causes of Congenital Heart Defects
The exact cause is often unknown, but several factors can increase risk.
Common Causes
- Genetic mutations
- Family history of heart defects
- Chromosomal abnormalities
- Maternal infections during pregnancy
- Poor maternal nutrition
- Alcohol or drug use during pregnancy
Genetic Heart Defects
Some heart defects are linked to inherited conditions. Genetic syndromes can increase the likelihood of heart abnormalities present at birth.
Signs of Heart Defect in Children
Symptoms depend on the type and severity of the condition.
Signs of Heart Defect
- Rapid breathing
- Poor feeding
- Fatigue during activity
- Sweating while feeding
- Slow growth or weight gain
- Bluish skin or lips
Heart Defect Symptoms in Newborns
- Difficulty breathing
- Low oxygen levels
- Weak pulse
- Lethargy
Early detection is critical to prevent complications.
Congenital Heart Failure
In some cases, congenital heart defects can lead to heart failure.
What Is Congenital Heart Failure
It occurs when the heart cannot pump blood efficiently due to structural problems.
Congenital Heart Failure Symptoms
- Rapid breathing
- Swelling in legs or abdomen
- Fatigue
- Poor feeding
- Frequent respiratory infections
Signs of Congenital Heart Failure
- Persistent cough
- Difficulty gaining weight
- Reduced activity levels
Congestive and Congenital Heart Failure
Congestive heart failure can develop as a complication of congenital defects.
- Fluid buildup in lungs and body
- Increased strain on the heart
- Requires immediate medical attention
Diagnosis of Congenital Heart Defects
Doctors use several methods to diagnose heart defects.
Common Diagnostic Tests
- Physical examination
- Echocardiogram
- Electrocardiogram
- Chest X-ray
- Pulse oximetry screening in newborns
Early screening helps detect defects even before symptoms appear.
Congenital Heart Failure Treatment
Treatment depends on the severity and type of defect.
Treatment Options
- Medications to manage symptoms
- Surgical repair of structural defects
- Catheter-based procedures
- Lifestyle modifications
Medications
- Drugs to improve heart function
- Diuretics to reduce fluid buildup
- Medications to control blood pressure
Surgical Treatment
- Corrective surgeries
- Valve repair or replacement
- Complex heart reconstruction
Management and Long-Term Care
Children with heart defects often require ongoing care.
Key Management Strategies
- Regular follow-up with a cardiologist
- Monitoring growth and development
- Maintaining a healthy diet
- Avoiding infections
With proper care, many children lead healthy lives.
Prevention of Congenital Heart Defects
Not all heart defects can be prevented, but certain measures reduce risk.
Preventive Measures
- Proper prenatal care
- Balanced nutrition during pregnancy
- Avoid alcohol and smoking
- Manage chronic conditions like diabetes
- Take recommended prenatal vitamins
When to See a Doctor
Seek medical attention if you notice:
- Difficulty breathing in a child
- Poor feeding or weight gain
- Bluish discoloration of skin
- Unusual fatigue
Early intervention can be life-saving.
Conclusion
Congenital heart defects are common but manageable conditions when detected early. Understanding the different types, symptoms, and treatment options empowers parents to make informed decisions.
Advancements in medical care have significantly improved outcomes, allowing many children with heart defects to live normal and fulfilling lives.
❓ FAQ: Congenital Heart Defects in Children
-
What are congenital heart defects in children?
Congenital heart defects (CHDs) are structural problems in the heart that are present at birth. These defects occur when the heart or blood vessels do not develop properly during pregnancy.
-
What are the most common types of congenital heart defects?
Some of the most common types include:
- Atrial Septal Defect (ASD)
- Ventricular Septal Defect (VSD)
- Patent Ductus Arteriosus (PDA)
- Tetralogy of Fallot
These conditions affect how blood flows through the heart and body.
-
What causes congenital heart defects in children?
The exact cause is often unknown, but possible factors include:
- Genetic conditions
- Maternal infections during pregnancy
- Certain medications
- Lifestyle factors like smoking or alcohol
Most defects develop during the early weeks of pregnancy when the baby’s heart is forming.
-
What are the symptoms of congenital heart defects in children?
Symptoms depend on the severity but may include:
- Bluish skin (cyanosis)
- Rapid breathing
- Poor feeding or weight gain
- Fatigue or shortness of breath
Some mild defects may not show symptoms until later in childhood.
-
How are congenital heart defects diagnosed?
Doctors may diagnose CHDs using:
- Ultrasound during pregnancy
- Physical examination after birth
- Echocardiogram (heart ultrasound)
- Pulse oximetry to check oxygen levels
Some defects are detected before birth, while others are found later.
-
Can congenital heart defects be treated?
Yes, treatment depends on the type and severity:
- Some mild defects may not need treatment
- Medications may help manage symptoms
- Procedures or surgery may be required
- In severe cases, a heart transplant may be needed
-
Can a child live a normal life with a congenital heart defect?
Many children with CHDs can live healthy and active lives, especially with early diagnosis and proper treatment. Advances in medical care have greatly improved outcomes.
-
Are congenital heart defects preventable?
Not all CHDs can be prevented, but risks can be reduced by:
- Proper prenatal care
- Managing maternal health conditions (like diabetes)
- Avoiding harmful substances during pregnancy
-
When should parents see a doctor?
You should consult a doctor if your child has:
- Difficulty breathing
- Poor weight gain
- Blue lips or skin
- Extreme tiredness
Early diagnosis can prevent complications.
-
Do congenital heart defects go away on their own?
Some minor defects, like small holes in the heart, may close naturally as the child grows. However, more serious defects usually require medical treatment or surgery.