Many women struggle with unexplained weight gain. They spend hours at the gym and eat clean diets. Yet, the scale does not move. For millions, the hidden culprit behind this battle is Polycystic Ovary Syndrome (PCOS). This common hormonal disorder affects up to ten percent of women of childbearing age.
Weight gain is one of the most frustrating symptoms of this condition. It usually settles around the belly. This stubborn fat leaves many women feeling defeated. They often blame themselves for a lack of willpower. However, the true cause is a complex web of hormonal imbalances.
Losing weight with this condition requires a different approach. Standard diet advice often fails. To find success, you must first understand your body. Let us explore the biological reasons behind this struggle and how you can manage them.
The Role of Insulin Resistance
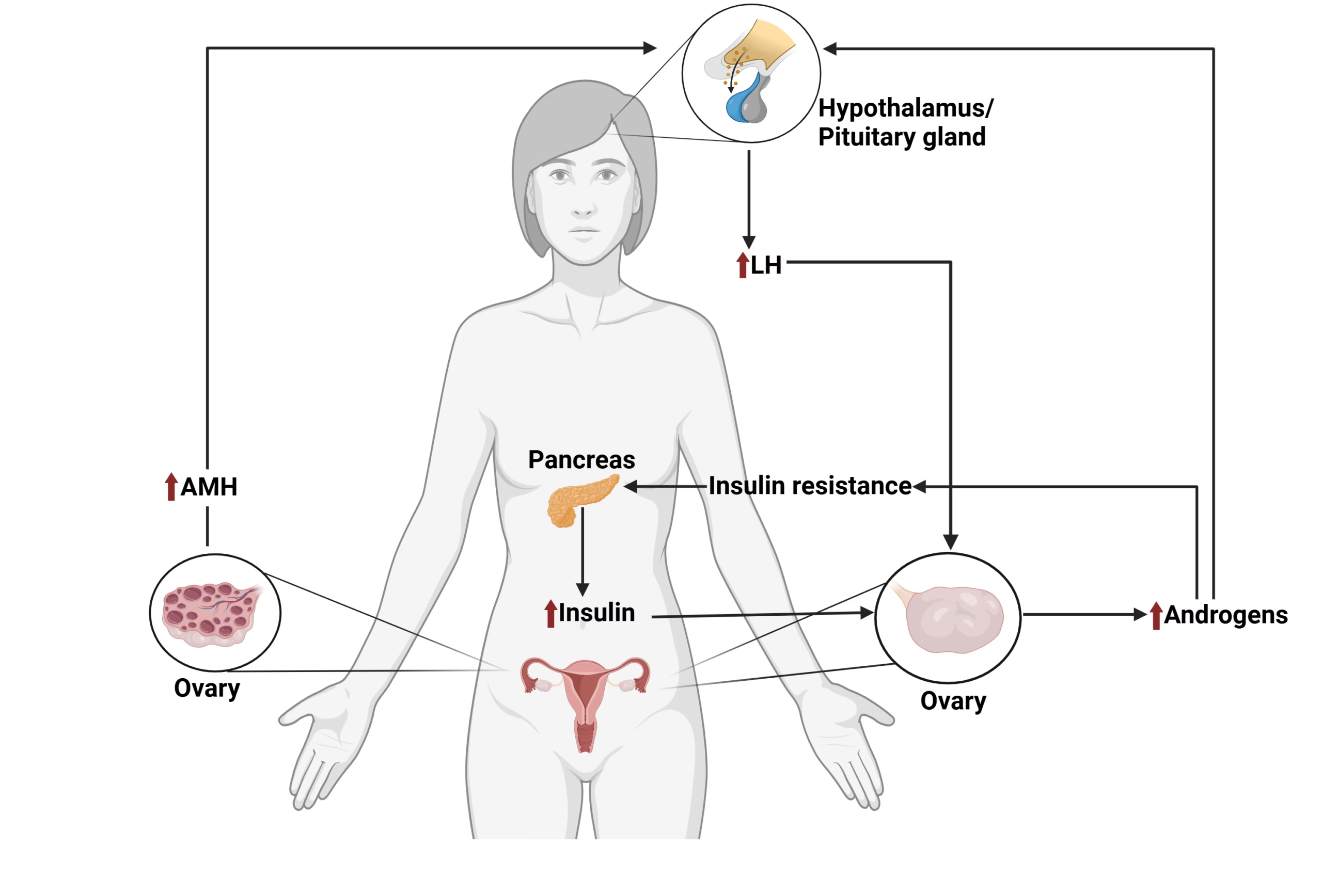
Insulin is a vital hormone made by your pancreas. It acts like a key. It unlocks your cells to let glucose enter and provide energy. When you have PCOS, your body’s cells often ignore this hormone. This condition is known as insulin resistance.
Because the cells are resistant, glucose stays in your bloodstream. Your pancreas panics and pumps out even more insulin. High levels of insulin tell your body to store fat. It also blocks your body from burning stored fat for fuel.
This process creates a frustrating cycle. Your cells crave energy because they cannot access glucose. This leads to intense cravings for sugar and carbohydrates. You eat more, your insulin spikes, and your body stores more fat.
High Androgens and Fat Storage
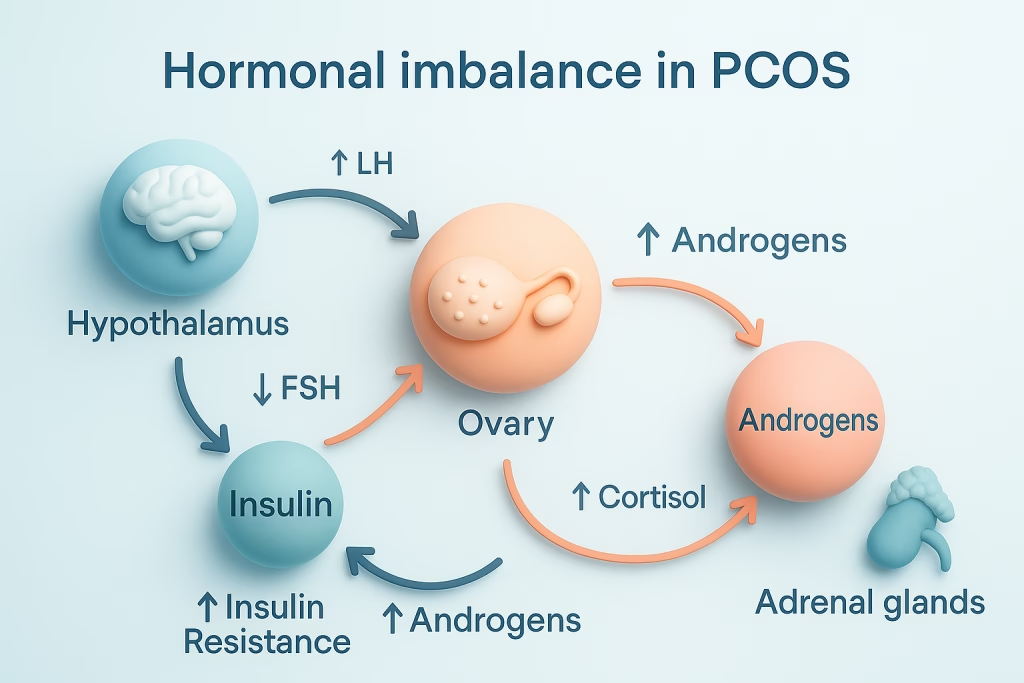
Women naturally produce small amounts of male hormones called androgens. Testosterone is one example. If you have PCOS, your ovaries produce higher levels of these hormones than normal. High insulin levels actually trigger this extra production.
Elevated androgens change how your body handles fat. Most women store fat in their hips and thighs. High androgen levels cause fat to accumulate in the abdomen instead. This is often called visceral fat or a PCOS belly.
Visceral fat is not just an appearance issue. It wraps around your vital internal organs. This type of fat is highly active. It increases inflammation and makes insulin resistance even worse over time.
The Slowed Metabolism Myth vs. Reality
Many women feel their metabolism is completely broken. Studies show that women with this condition often have a lower basal metabolic rate. This means your body naturally burns fewer calories at rest than someone without the condition.
Your body is essentially programmed to conserve energy. It acts as if it is in survival mode. A normal calorie deficit might not work for you. Your body adapts quickly to lower food intake by slowing down further.
This lower metabolic rate makes traditional weight loss formulas inaccurate. Tracking calories alone rarely works. You must focus on changing your hormonal landscape to kickstart your metabolism instead.
Hunger Hormones Out of Balance
Your body uses specific hormones to signal hunger and fullness. Ghrelin tells your brain when it is time to eat. Leptin signals your brain when you are full. In a healthy body, these hormones keep your appetite stable.
PCOS disrupts this delicate balance completely. Research shows that ghrelin levels do not drop properly after a meal. You might finish a large dinner and still feel physically hungry an hour later.
At the same time, your body can become resistant to leptin. Your brain stops receiving the message that you have enough energy. This hormonal confusion leaves you fighting constant physical hunger every day.
Chronic Inflammation and Weight Gain
Living with this condition means your body experiences low-grade chronic inflammation. Your immune system is constantly on high alert. Doctors can measure this through specific proteins in your blood.
Inflammation and weight gain feed into each other. Inflammatory signals interfere with insulin receptors on your cells. This worsens insulin resistance. As a result, your body stores more fat in response.
Fat cells then produce their own inflammatory chemicals. This creates a dangerous loop. The more fat your body stores, the more inflamed it becomes. This makes weight loss even harder to achieve.
The Impact of Stress and Cortisol
Dealing with chronic symptoms is highly stressful. Stress triggers your adrenal glands to produce cortisol. Cortisol is your body’s primary stress hormone. High levels of cortisol are directly linked to weight gain.
Cortisol encourages your body to hold onto fat. It specifically targets the abdominal area. It also raises blood sugar levels. This gives your body a quick burst of energy that you do not use.
When this energy is not used, insulin stores it as fat. High cortisol also drives cravings for comfort foods. These foods are usually high in fat and sugar, which feeds the cycle.
Sleep Disturbances and Fat Loss
Sleep is essential for healthy hormone regulation. Women with this condition are at a much higher risk for sleep issues. Sleep apnea is common due to airway inflammation and weight.
Poor sleep disrupts your hunger hormones. Just one night of bad sleep increases ghrelin. It also decreases leptin the following day. This makes you crave high-calorie foods for quick energy.
Lack of sleep also worsens insulin resistance immediately. Your body cannot process glucose efficiently when it is exhausted. Prioritizing rest is a critical part of any successful weight management plan.
Why Traditional Diet Advice Fails
Most standard diet plans rely on extreme calorie restriction. They often advocate for hours of intense cardio exercise. While this works for some, it often backfires for women with PCOS.
Severe calorie restriction acts as a major stressor. It raises your cortisol levels significantly. Intense cardio can also spike cortisol. This tells your body to hold onto its fat stores even tighter.
Cutting out entire food groups can trigger intense binges. This happens because your hunger hormones are already unstable. A sustainable approach must focus on nourishment rather than deprivation.
Smart Dietary Strategies for Success
To lose weight, you must focus on balancing your blood sugar. Avoid extreme low-calorie diets. Instead, build your meals around three main pillars: protein, healthy fats, and fiber.
- Prioritize Protein: Eat protein with every meal. Lean meats, fish, eggs, and tofu help stabilize blood sugar. Protein also keeps you feeling full for longer periods.
- Choose Complex Carbs: Do not cut out carbs completely. Swap refined carbs for whole options. Vegetables, berries, quinoa, and legumes digest slowly and prevent insulin spikes.
- Include Healthy Fats: Avocados, nuts, seeds, and olive oil are essential. They slow down digestion. They also support healthy hormone production in your body.
The Right Way to Exercise
Exercise is crucial, but type and intensity matter. Long, grueling cardio sessions can raise stress hormones. Focus on workouts that improve insulin sensitivity without exhausting your body.
- Strength Training: Lift weights or use bodyweight exercises. Building muscle mass improves your metabolic rate. Muscle cells use glucose for fuel efficiently, even at rest.
- Walking: Never underestimate the power of a daily walk. A 20-minute walk after meals lowers blood sugar spikes. It is also an excellent way to lower cortisol.
- HIIT in Moderation: High-Intensity Interval Training can be beneficial. Keep these sessions short. Limit them to twice a week to avoid overstressing your system.
The Importance of Lifestyle and Supplements
Diet and exercise are only part of the puzzle. Managing stress is just as important. Practice regular stress-relief techniques. Meditation, deep breathing, and yoga can significantly lower cortisol levels.
Specific supplements can also support your journey. Always speak with your doctor before starting any new routine. Some options have strong scientific backing for managing symptoms.
- Inositol: This supplement helps improve insulin sensitivity. It can reduce sugar cravings and help regulate your ovulation cycle.
- Omega-3 Fatty Acids: High-quality fish oil reduces chronic inflammation. It also helps improve cholesterol profiles.
- Vitamin D: Many women with this condition are deficient. Vitamin D is essential for insulin management and overall immune function.
Shifting Your Mindset
Weight loss with this condition takes time. It is a slow, gradual process. Expecting rapid results will only lead to frustration. Celebrate small victories that do not involve the scale.
Notice if your energy levels are improving. Track changes in your skin, mood, and sleep quality. These are signs that your hormones are shifting in a positive direction.
Be kind to yourself during this process. Your body is not working against you maliciously. It is dealing with a complex hormonal challenge. It needs your patience, care, and consistent support.
If you’d like to know more about how PCOS symptoms, then please check our detailed article – PCOS Symptoms Before Diagnosis.
Frequently Asked Questions (FAQs)
Can you actually lose weight if you have PCOS?
Yes. Weight loss is possible, but it requires balancing your hormones first rather than just cutting calories. Focus on managing insulin levels and lowering your daily stress.
Why does PCOS cause fat to store mainly in the stomach?
High levels of male hormones, called androgens, alter where your body stores fat. Instead of storing it in the hips, your body deposits fat in the abdomen, creating visceral fat.
Does cutting out all carbohydrates fix PCOS weight gain?
No, you do not need to cut out all carbohydrates. Focus on replacing refined carbs with high-fiber complex carbohydrates, which prevent drastic insulin spikes.
How long does it take to see weight loss results with PCOS?
Results vary for everyone, but sustainable hormone healing takes time. Most women start seeing real, lasting changes within three to six months of consistent lifestyle changes.