You are tired all the time. Your periods are all over the place. You are gaining weight without changing anything. Your hair is thinning. Your mood feels off.
You search your symptoms online and land on two possible answers — PCOS or a thyroid disorder. Both seem to fit. Both involve hormones. Both affect your cycle, your weight, and your energy.
So which one is it?
This guide breaks down the key differences between PCOS and thyroid disorders. It covers how each condition works, which symptoms overlap, which symptoms are unique to each, and how doctors tell them apart.
What Is PCOS
PCOS stands for Polycystic Ovary Syndrome. It is a hormonal condition that affects the ovaries. In PCOS, the body produces too much androgen — a type of male hormone. This disrupts ovulation and causes a wide range of symptoms.
PCOS affects between 8% and 13% of women of reproductive age. Many go undiagnosed for years because the symptoms vary so much from person to person.
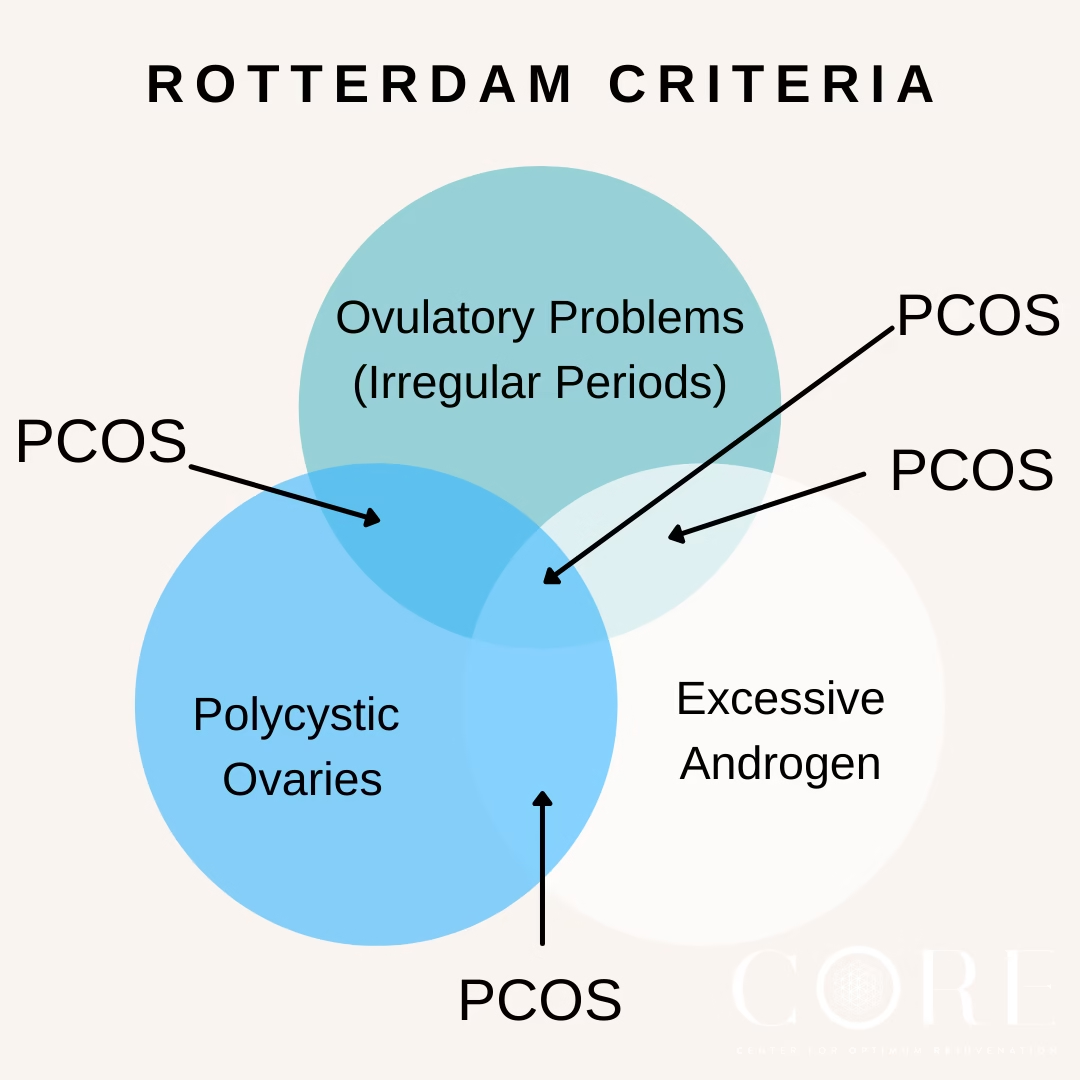
The three main features of PCOS are:
- Irregular or absent periods caused by disrupted ovulation
- Signs of excess androgen — such as acne, facial hair, or hair thinning on the scalp
- Polycystic ovaries visible on an ultrasound scan
You do not need all three to be diagnosed. Two out of three is enough.
What Is a Thyroid Disorder
The thyroid is a small, butterfly-shaped gland in your neck. It produces hormones that control your metabolism — the rate at which your body uses energy. When the thyroid is not working properly, everything slows down or speeds up.
There are two main types of thyroid disorder:
- Hypothyroidism — the thyroid is underactive and produces too little hormone. This is the more common type and shares the most overlap with PCOS.
- Hyperthyroidism — the thyroid is overactive and produces too much hormone. This causes a different set of symptoms including rapid heartbeat, weight loss, and anxiety.
Hypothyroidism is the type most often confused with PCOS. The rest of this guide focuses primarily on that comparison.
Why These Two Conditions Get Confused
Both PCOS and hypothyroidism affect women more than men. Both are hormonal conditions. Both cause irregular periods, weight changes, fatigue, and hair loss.
When you look at just the surface symptoms, they can feel almost identical. This is why so many women get misdiagnosed — or spend months trying to figure out which condition they are dealing with.
The confusion goes even deeper. PCOS and thyroid disorders can occur together. Having one does not protect you from having the other. Some women are managing both at the same time without knowing it.
Symptoms That Overlap
These symptoms appear in both PCOS and thyroid disorders:
- Irregular or missed periods
- Weight gain or difficulty losing weight
- Fatigue and low energy
- Hair thinning or hair loss
- Mood changes, anxiety, or depression
- Difficulty concentrating or brain fog
- Dry skin
Looking at this list alone, it is impossible to tell which condition you have. This is exactly why blood tests are necessary — symptoms alone cannot give you an answer.
Symptoms That Point More Toward PCOS
Some symptoms are far more common in PCOS than in thyroid disorders. These are driven by excess androgen, which is specific to PCOS.
Watch for these signs:
- Excess facial or body hair — on the chin, upper lip, chest, or stomach
- Acne along the jawline, chin, or cheeks — especially in adulthood
- Hair thinning specifically at the crown or parting of the scalp
- Dark patches of skin on the neck, armpits, or inner thighs
- Irregular periods that have always been unpredictable — not a recent change
- Difficulty getting pregnant due to irregular ovulation
- Ovarian cysts visible on ultrasound
If you have several of these alongside the overlapping symptoms, PCOS is more likely the primary issue. However, a thyroid problem can still coexist and should be ruled out.
Symptoms That Point More Toward Thyroid Disorder
Signs of Hypothyroidism (Underactive Thyroid)
These symptoms suggest the thyroid rather than PCOS:
- Feeling cold all the time — especially cold hands and feet
- Constipation or very slow digestion
- Puffy face, particularly around the eyes in the morning
- Slow heart rate
- Voice becoming hoarser or deeper
- Muscle weakness or cramping
- A visible swelling at the front of the neck (called a goitre)
- Periods that become very heavy — not just irregular
- Extreme fatigue that does not improve with rest
Signs of Hyperthyroidism (Overactive Thyroid)
If your thyroid is overactive, the symptoms look very different:
- Rapid or irregular heartbeat (palpitations)
- Unexplained weight loss despite eating normally
- Feeling hot and sweating more than usual
- Trembling hands
- Nervousness and restlessness
- Frequent bowel movements
- Bulging eyes (in Graves’ disease, the most common cause of hyperthyroidism)
Hyperthyroidism is less commonly confused with PCOS because the symptoms are distinct. Weight loss and a racing heart are not typical PCOS features.
Key Hormonal Differences
This is where the two conditions become clearly distinct. The hormones involved are completely different.
Hormones in PCOS
PCOS involves:
- Elevated androgens — testosterone or DHEA-S above normal range
- A higher LH to FSH ratio than normal
- Elevated insulin, often linked to insulin resistance
- Normal thyroid hormones in most cases
Hormones in Thyroid Disorder
Thyroid disorders involve:
- Elevated TSH (thyroid stimulating hormone) in hypothyroidism — the pituitary works harder to stimulate a sluggish thyroid
- Low TSH in hyperthyroidism — the pituitary backs off when the thyroid is overproducing
- Low T3 and T4 (active thyroid hormones) in hypothyroidism
- High T3 and T4 in hyperthyroidism
- Normal androgen levels in most cases
A simple blood test measuring TSH, T3, and T4 is enough to confirm or rule out a thyroid disorder. This is one of the first tests a doctor should run when PCOS symptoms are present.
How Doctors Tell Them Apart
Blood Tests
Your doctor will run a panel that covers both conditions. Key tests include:
- TSH, free T3, free T4 — confirms or rules out thyroid dysfunction
- Total and free testosterone, DHEA-S — checks for androgen excess pointing to PCOS
- LH and FSH ratio — often elevated in PCOS
- Fasting insulin and glucose — checks for insulin resistance common in PCOS
- Full blood count and ferritin — rules out anaemia, which can also cause fatigue and hair loss
Pelvic Ultrasound
This scan checks the ovaries for the follicle pattern associated with PCOS. A thyroid disorder does not affect the ovaries, so a polycystic appearance on ultrasound points strongly toward PCOS.
Thyroid Ultrasound
If a thyroid disorder is suspected, a doctor may order a thyroid ultrasound or a thyroid antibody test. This checks for autoimmune thyroid conditions like Hashimoto’s thyroiditis, which is the most common cause of hypothyroidism.
Can You Have Both at the Same Time
Yes — and this is more common than most people realise.
Research shows that thyroid disorders occur more frequently in women with PCOS than in the general population. Hashimoto’s thyroiditis in particular has a higher prevalence among women with PCOS.
Why This Happens
Both conditions involve immune system activity and hormonal disruption. The exact connection is still being studied. But the practical implication is important — if you have PCOS, your doctor should still test your thyroid function regularly. A thyroid problem on top of PCOS can significantly worsen symptoms like fatigue, weight gain, and irregular periods.
What to Do If You Have Both
Managing both conditions at the same time is very possible. Most women with both PCOS and hypothyroidism take thyroid medication (typically levothyroxine) to normalise thyroid hormone levels, alongside PCOS-specific lifestyle and medical interventions.
Treating the thyroid condition often improves some PCOS symptoms as well — particularly fatigue and cycle irregularity.
A Simple Way to Think About It
If you are trying to make sense of your symptoms before a doctor’s appointment, think about it this way.
PCOS tends to show up as androgen-driven symptoms — acne, facial hair, scalp hair thinning, irregular periods that have always been unpredictable, and signs of insulin resistance like sugar cravings and abdominal weight gain.
A thyroid disorder tends to show up as metabolism-driven symptoms — feeling cold, constipation, puffiness, very slow or very fast heart rate, and periods that changed recently rather than always being irregular.
But because the overlap is real and both can occur together, you need blood tests to know for certain. Guessing based on symptoms alone is not enough.
What to Ask Your Doctor
Go into your appointment prepared. Ask your doctor to test for both conditions at the same time. There is no reason to test one and assume the other is fine.
Ask for:
- A full thyroid panel — TSH, free T3, free T4, and thyroid antibodies
- Hormone panel — testosterone, DHEA-S, LH, FSH
- Metabolic tests — fasting insulin and fasting glucose
- A pelvic ultrasound if PCOS is suspected
Getting a clear picture from the start saves months of confusion and back-and-forth appointments.
Frequently Asked Questions
Can a thyroid disorder cause PCOS?
A thyroid disorder does not directly cause PCOS. However, hypothyroidism can disrupt the menstrual cycle and raise prolactin levels, which can mimic PCOS symptoms closely. This is why doctors rule out thyroid issues before confirming a PCOS diagnosis.
Can PCOS affect the thyroid?
PCOS does not directly damage the thyroid. But women with PCOS have a higher rate of autoimmune thyroid conditions like Hashimoto’s thyroiditis. The connection is not fully understood, but regular thyroid testing is recommended for women with PCOS.
What is the fastest way to tell PCOS from a thyroid disorder?
A blood test. TSH measures thyroid function. Testosterone and DHEA-S measure androgen levels. These two tests together give a clear picture of which condition — or both — may be present.
I have regular periods. Can I still have PCOS?
Yes. Some women with PCOS have regular periods but still meet the other two Rotterdam Criteria — elevated androgens and polycystic ovaries on ultrasound. Regular periods alone do not rule out PCOS.
My TSH came back normal but I still feel terrible. What now?
A normal TSH does not mean all thyroid hormones are optimal. Ask your doctor to also test free T3 and free T4. Some women feel symptoms at TSH levels that fall within the standard range. If thyroid results are all normal, PCOS or another hormonal condition may be the cause.
Which condition is easier to treat?
Both are very manageable with the right approach. Hypothyroidism is often treated with a daily thyroid hormone replacement tablet, which most people tolerate well. PCOS management involves more lifestyle elements — diet, exercise, sleep, and sometimes medication — and requires a more personalised approach.
This content is for informational purposes only and does not replace professional medical advice. Always consult a qualified healthcare provider for a proper diagnosis and treatment plan.
For the complete guide to understanding and managing PCOS, see: The Complete Guide to PCOS.