
Getting a PCOS diagnosis can feel like a long, frustrating journey. Many women visit multiple doctors before anyone takes their symptoms seriously. Others get a diagnosis but never fully understand how the doctor reached that conclusion.
If you suspect you have PCOS, knowing what the diagnostic process looks like puts you in a stronger position. You will know what to ask for, what tests to expect, and why no single test can confirm PCOS on its own.
This guide walks you through the entire process — from your first appointment to getting a confirmed diagnosis.
Why PCOS Is Hard to Diagnose
PCOS does not show up on one simple test. There is no blood marker that says “yes, you have PCOS.” Doctors diagnose it by looking at a combination of symptoms, test results, and ruling out other conditions.
This is why diagnosis can take time. Two women with PCOS can have completely different symptoms. One may have irregular periods and acne. Another may have regular periods but elevated testosterone and polycystic ovaries on a scan.
The process requires patience. But once you understand the steps, it becomes much less overwhelming.
Step One — Visiting Your Doctor
What to Bring to Your First Appointment
Your first appointment sets the tone for everything that follows. Come prepared. Bring a written summary of your symptoms, even if they seem unrelated to each other.
Be ready to discuss:
- Your menstrual cycle history — how long, how regular, how heavy
- Any changes in your skin, hair, or weight
- Family history of PCOS, diabetes, or hormonal conditions
- Any medications or supplements you currently take
Do not downplay your symptoms. Many women describe feeling dismissed at first appointments. Being specific and prepared makes it harder for concerns to be brushed aside.
What the Doctor Will Ask You
Your doctor will likely ask how long you have had symptoms and whether they have changed over time. They will ask about your periods — whether they are irregular, absent, or very heavy. They may also ask about stress levels, diet, and any previous diagnoses.
This conversation matters. It helps the doctor decide which tests to order next.
Step Two — The Physical Examination
A physical exam checks for visible signs of androgen excess. This is the term for higher-than-normal levels of male hormones like testosterone.
Your doctor may look for:
- Acne, especially along the jawline and chin
- Excess hair on the face, chest, or stomach (called hirsutism)
- Hair thinning on the scalp
- Dark patches of skin on the neck, armpits, or groin (called acanthosis nigricans)
- Weight distribution, particularly around the abdomen
These physical signs give the doctor valuable clues. They help narrow down whether androgen excess is playing a role in your symptoms.
Step Three — Blood Tests
Blood tests are a core part of diagnosing PCOS. They help confirm hormonal imbalances and rule out other conditions that can mimic PCOS symptoms.
Hormone Tests
Your doctor will likely test:
- Testosterone (total and free) — elevated levels point toward androgen excess
- LH and FSH ratio — women with PCOS often have a higher LH to FSH ratio than normal
- DHEA-S — an androgen produced by the adrenal glands, elevated in some types of PCOS
- Prolactin — to rule out a pituitary gland problem
- AMH (anti-Müllerian hormone) — often elevated in PCOS, reflects the number of follicles present
Metabolic Tests
Because insulin resistance is present in up to 70% of women with PCOS, these tests are important:
- Fasting insulin and fasting glucose — checks how well your body handles blood sugar
- HbA1c — a longer-term marker of blood sugar regulation
- Lipid panel — checks cholesterol levels, which can be affected by PCOS
Thyroid Tests
Thyroid conditions can cause irregular periods and weight changes — just like PCOS. Your doctor will test TSH (thyroid stimulating hormone) to rule this out before confirming a PCOS diagnosis.
Step Four — Pelvic Ultrasound
A pelvic ultrasound lets the doctor look directly at your ovaries and uterus. It checks for the characteristic follicle pattern associated with PCOS.
What the Ultrasound Looks For
The doctor or sonographer will check:
- The number of follicles in each ovary
- The size of the ovaries
- The appearance and thickness of the uterine lining
In PCOS, the ovaries often contain multiple small follicles arranged around the outer edge. This is sometimes described as a “string of pearls” appearance. The current threshold used in many guidelines is twelve or more follicles per ovary, or an ovarian volume greater than ten millilitres.
Transvaginal vs Abdominal Ultrasound
A transvaginal ultrasound — where a small probe is gently inserted into the vagina — gives a clearer image of the ovaries. An abdominal ultrasound is performed externally and may be used for women who prefer it or for those who have not been sexually active.
Both are safe. Your doctor will discuss which option is more appropriate for you.
One Important Note
You can have PCOS without polycystic ovaries on ultrasound. And you can have follicles on ultrasound without having PCOS. The scan is one piece of the puzzle — not the whole picture.
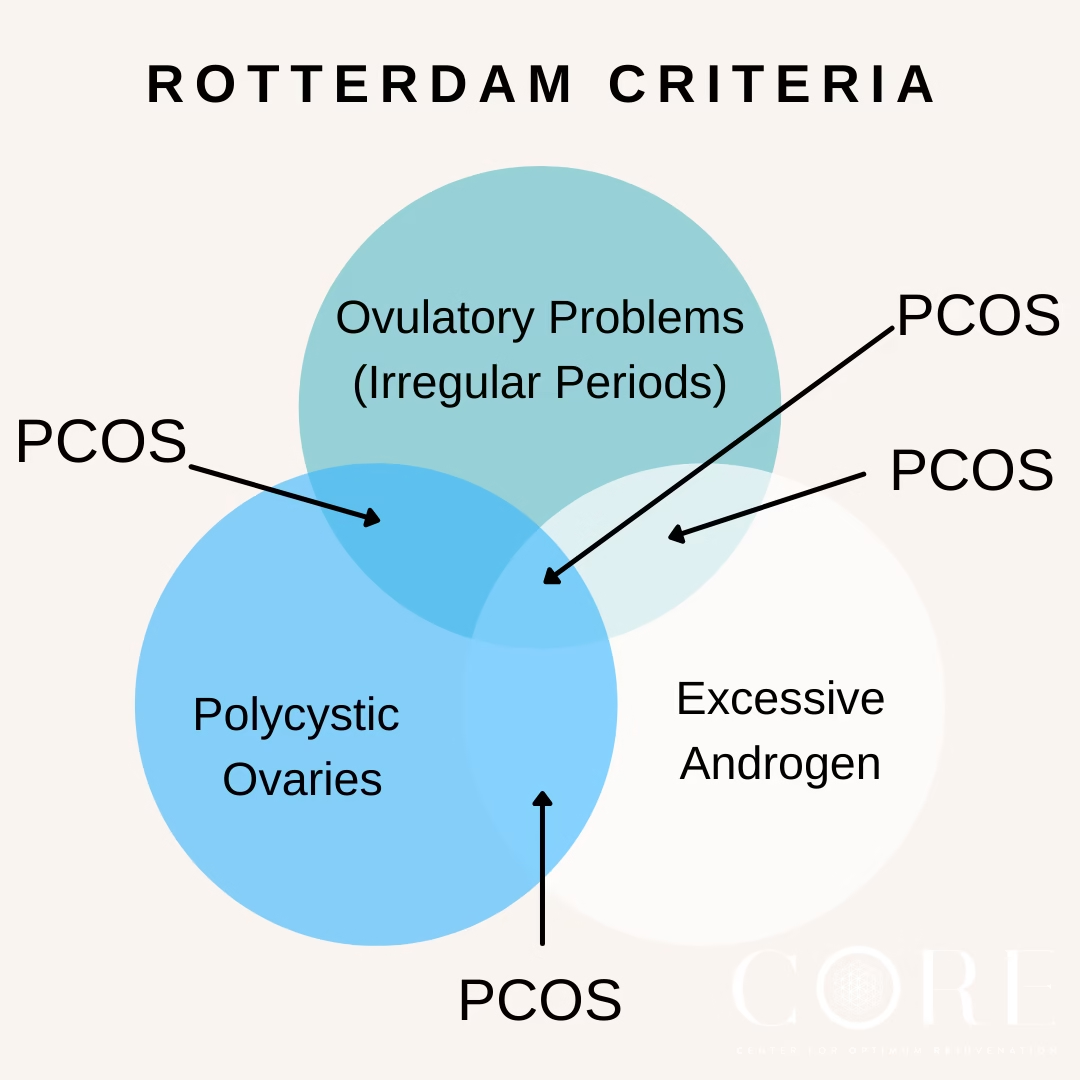
Step Five — The Rotterdam Criteria
This is the framework doctors use to make a formal PCOS diagnosis. It was established at a 2003 consensus meeting in Rotterdam and remains the most widely used diagnostic standard worldwide.
What the Rotterdam Criteria Requires
To receive a PCOS diagnosis, you need to meet at least two of these three criteria:
- Irregular or absent ovulation — usually reflected in irregular or missing periods
- Clinical or biochemical signs of androgen excess — either visible symptoms like acne and hirsutism, or elevated androgens on blood tests
- Polycystic ovaries on ultrasound — meeting the follicle count or volume threshold
You do not need all three. Two out of three is sufficient for a diagnosis.
Why This Matters for You
Because only two criteria are needed, PCOS can present in several different combinations. This is why the condition looks so different from person to person. It also explains why some women with PCOS have regular periods, or why some have no visible cysts on ultrasound.
Step Six — Ruling Out Other Conditions
Before confirming PCOS, doctors need to rule out other conditions that cause similar symptoms. This step is essential and sometimes overlooked.
Conditions that can mimic PCOS include:
- Thyroid disorders — hypothyroidism causes weight gain, fatigue, and irregular periods
- Hyperprolactinemia — elevated prolactin from a pituitary issue can disrupt periods and cause acne
- Congenital adrenal hyperplasia (CAH) — a genetic condition that causes excess androgen production
- Cushing’s syndrome — a condition involving excess cortisol, with symptoms that overlap significantly with PCOS
- Premature ovarian insufficiency — causes irregular or absent periods in younger women
Your doctor will use your blood test results and medical history to work through this list. Ruling these out is what makes a PCOS diagnosis reliable.
What Happens After Diagnosis
Getting a Clear Explanation
Once diagnosed, ask your doctor to explain which criteria you met. Understanding whether your PCOS involves androgen excess, irregular ovulation, or polycystic ovaries — or a combination — helps you understand your specific type and what drives your symptoms.
Discussing Next Steps
There is no cure for PCOS, but it is very manageable. Your doctor should discuss:
- Lifestyle changes — diet and exercise that target insulin resistance
- Medication options — depending on your main symptoms and whether you want to conceive
- Monitoring — what to track and how often to follow up
If you feel your concerns are being dismissed or your diagnosis feels rushed, it is completely reasonable to seek a second opinion. A gynaecologist or endocrinologist who specialises in PCOS will offer a more thorough assessment.
Diagnosing PCOS in Teenagers
Diagnosing PCOS in adolescents requires extra care. Irregular periods and mild acne are normal during early puberty. This makes it difficult to separate typical teenage hormonal changes from genuine PCOS.
Most guidelines recommend waiting at least two years after the first period before making a PCOS diagnosis in a teenager. The same Rotterdam Criteria apply, but doctors apply them more cautiously in younger patients.
If you are a parent concerned about a teenager’s symptoms, raise it with a doctor — but expect a longer observation period before a formal diagnosis is given.
Frequently Asked Questions
Can a doctor diagnose PCOS from symptoms alone?
No. Symptoms give important clues, but a formal diagnosis requires meeting the Rotterdam Criteria. This means at least two of the three criteria must be confirmed through examination, blood tests, or ultrasound.
Do I need an ultrasound to be diagnosed with PCOS?
Not necessarily. If you already meet the first two Rotterdam criteria — irregular ovulation and signs of androgen excess — a diagnosis can be made without an ultrasound. However, most doctors will recommend one to get a complete picture.
Can PCOS be diagnosed during a regular period?
Yes. Irregular periods are one criterion, not a requirement. Women with regular periods can still be diagnosed with PCOS if they meet the other two criteria.
What if my blood tests come back normal?
Normal blood tests do not rule out PCOS. Some women with PCOS have testosterone levels within the standard range. This is why the Rotterdam Criteria looks at the full combination — not any single result.
How long does it take to get a PCOS diagnosis?
It varies widely. Some women get a diagnosis within one or two appointments. Others take months or years, particularly if symptoms are mild or if previous doctors did not consider PCOS. Bringing a written symptom history to your appointment can speed up the process significantly.
Should I see a gynaecologist or a GP first?
Starting with your GP is fine. They can order the initial blood tests and ultrasound. If the results are complex or your symptoms are severe, your GP can refer you to a gynaecologist or endocrinologist for a more detailed evaluation.
This content is for informational purposes only and does not replace medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.
For the full picture of PCOS including types, causes, and treatment, see our main guide: The Complete Guide to PCOS.