The Complete Guide to PCOS: Symptoms, Causes, Types, and Treatment
Polycystic Ovary Syndrome is one of the most common hormonal conditions affecting women of reproductive age — and one of the most misunderstood. It is estimated to affect between 8% and 13% of women worldwide, yet millions go undiagnosed for years, cycling through frustrating symptoms without a clear explanation.
This guide is the most complete resource on this site for understanding PCOS. It covers what the condition actually is, why it happens, how it shows up differently in different women, how it is diagnosed, and what genuine management looks like — both medically and through lifestyle. Every major section links out to a dedicated in-depth guide so you can go as deep as you need on any specific aspect of the condition.
If you have recently been diagnosed, if you suspect you might have PCOS, or if you simply want to understand the condition more thoroughly, start here.
Table of Contents
- What Is PCOS
- PCOS vs PCOD — What Is the Difference
- The 4 Types of PCOS
- How PCOS Affects Your Entire Body
- Common Symptoms of PCOS
- Hidden and Overlooked Symptoms
- What Causes PCOS
- How PCOS Is Diagnosed
- PCOS and Mental Health
- PCOS and Diet and Nutrition
- PCOS and Fertility
- Treatment Options for PCOS
- Long-Term Health Risks of PCOS
- Living Well With PCOS
- Frequently Asked Questions
What Is PCOS?
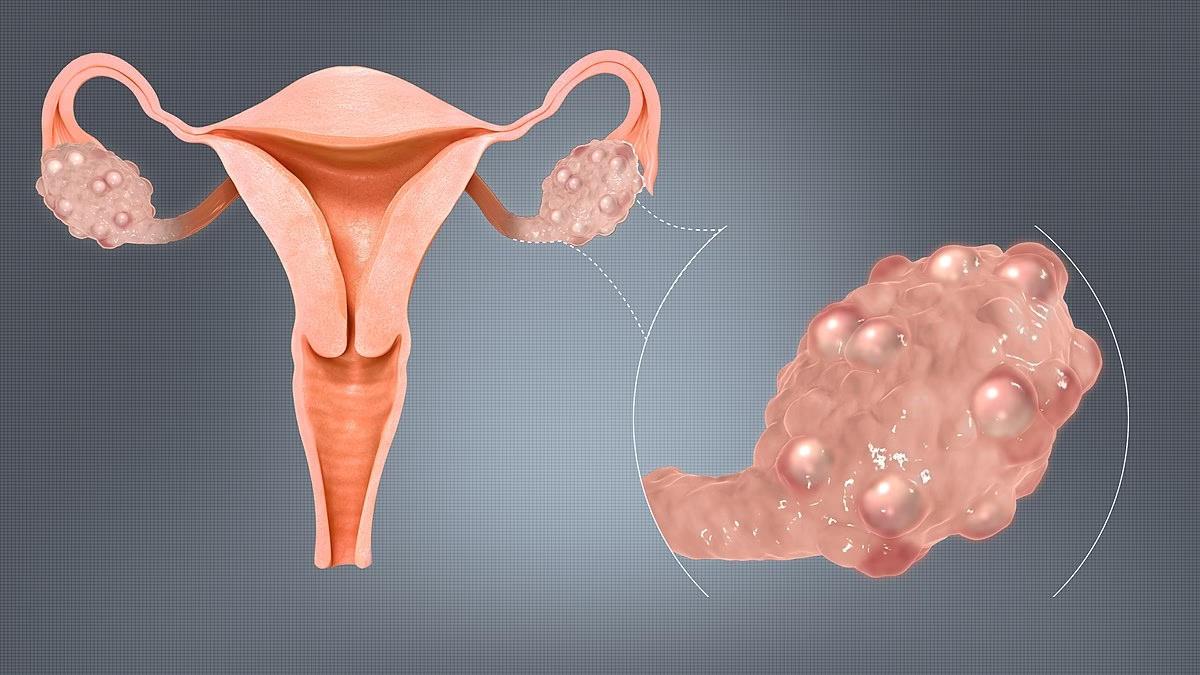
PCOS (Polycystic Ovary Syndrome) is a hormonal disorder in which the ovaries produce an abnormal amount of androgens — often called male hormones — disrupting the normal process of ovulation. This imbalance can lead to irregular or absent menstrual cycles, the development of multiple small follicles in the ovaries, and a wide range of symptoms that extend far beyond reproductive health.
Despite its name, you do not need to have ovarian cysts to be diagnosed with PCOS. The cysts described in the name are not true cysts — they are immature follicles that failed to release an egg and collected in the ovary. Many women diagnosed with PCOS have no visible follicles on ultrasound, while some women with follicles on ultrasound do not have the condition.
PCOS is not a single, uniform disease. It is a syndrome — meaning it presents differently from person to person depending on which underlying mechanisms are driving it. This is why treatment that works well for one woman may do little for another, and why understanding your specific type matters.
PCOS vs PCOD — What Is the Difference
These two terms are frequently confused, and in some regions used interchangeably, but they refer to different things.
PCOD (Polycystic Ovary Disease) refers specifically to a structural finding — the presence of multiple cysts in the ovaries. It is considered a milder condition in which the ovaries release immature eggs that accumulate as cysts. Lifestyle changes alone can often manage PCOD effectively, and it does not always cause the same degree of hormonal disruption.
PCOS is a broader endocrine disorder involving hormonal imbalance, disrupted ovulation, and androgen excess. It has wider systemic effects on metabolism, mental health, cardiovascular health, and fertility. PCOS typically requires more comprehensive management.
A woman can have PCOD without PCOS, but PCOS generally includes the ovarian changes associated with PCOD alongside more significant hormonal disruption.
The 4 Types of PCOS
Not all PCOS cases are driven by the same underlying mechanism. Understanding which type you are dealing with is one of the most important steps toward effective management, because the root cause shapes both the symptoms and the best response.
Insulin-Resistant PCOS
This is the most common type, affecting the majority of women with PCOS. It occurs when the body’s cells stop responding efficiently to insulin, causing the pancreas to produce more. Elevated insulin levels signal the ovaries to produce excess androgens, which disrupts ovulation and triggers the characteristic symptoms of PCOS.
Typical signs include difficulty losing weight, intense sugar cravings, energy crashes after meals, fatigue, irregular periods, and dark patches of skin on the neck or underarms (a condition called acanthosis nigricans). Women with this type have a higher risk of developing type 2 diabetes over time.
Inflammatory PCOS
In this type, chronic low-grade inflammation drives androgen production. The inflammation can be triggered by dietary factors, gut health issues, environmental toxins, or an underlying autoimmune response. The immune system remains in a low-level state of activation that continuously stimulates the ovaries.
Symptoms often include persistent fatigue, unexplained headaches, skin issues, joint discomfort, and digestive problems alongside the hormonal symptoms of PCOS. Blood tests may show elevated inflammatory markers such as CRP (C-reactive protein).
Adrenal PCOS
Adrenal PCOS is driven not by the ovaries but by the adrenal glands. When the adrenal glands are under chronic stress, they overproduce androgens — particularly DHEA-S (dehydroepiandrosterone sulfate) — independently of insulin levels.
This type is often seen in women under significant and prolonged stress, and is closely connected to HPA axis dysregulation. Unlike insulin-resistant PCOS, women with adrenal PCOS often have normal insulin levels, normal weight, and may not respond to the dietary interventions that help other types. Stress management, nervous system regulation, and adrenal support are central to managing this type.
Post-Pill PCOS
This type can emerge after stopping hormonal contraceptives. Birth control pills suppress the body’s natural hormone production. When they are discontinued, the hormonal system must restart — and for some women, this recalibration process goes wrong, producing a temporary surge in androgens and PCOS-like symptoms.
Symptoms typically include irregular periods, acne, and hair shedding in the months following discontinuation. In many cases, post-pill PCOS resolves on its own within three to six months. However, for some women the underlying hormonal dysregulation was already present before the pill and was simply being masked by it.
For a complete breakdown of all four types including how to identify which one applies to you, see our dedicated guide: The 4 Types of PCOS Explained.
How PCOS Affects Your Entire Body
PCOS is not a condition confined to the ovaries. It is a full-body endocrine disorder that affects multiple systems simultaneously.
Hormonal System
The hormonal disruption in PCOS is multidimensional. Elevated androgens suppress normal ovulation. LH (luteinizing hormone) levels are often disproportionately high relative to FSH (follicle-stimulating hormone), throwing off the signals the ovaries need to release eggs regularly. In some women, cortisol and prolactin are also affected. This is why symptoms can appear across so many apparently unrelated areas — the hormonal system influences nearly every function in the body.
Metabolic System
Insulin resistance is present in up to 70% of women with PCOS, regardless of body weight. When the body produces excess insulin to compensate, it fuels a cycle of fat storage (particularly around the abdomen), increased androgen production, and energy dysregulation. Over time, this metabolic disruption significantly raises the risk of type 2 diabetes, fatty liver disease, and metabolic syndrome.
Reproductive System
PCOS directly impairs the ovulation process. When ovulation is irregular or absent, the uterine lining does not shed normally, leading to irregular or missed periods. Immature follicles may accumulate in the ovaries. The combination of anovulation (absent ovulation) and hormonal imbalance is the primary reason PCOS is one of the leading causes of female infertility — though it is important to note that many women with PCOS conceive successfully with appropriate support.
Skin and Hair
Excess androgens cause several visible changes. Acne — particularly along the jawline, chin, and cheeks — is one of the most common presenting symptoms. Hirsutism (excess hair growth on the face, chest, or back) affects a significant proportion of women with PCOS. Simultaneously, androgenic alopecia (hair thinning on the scalp) can occur. Skin darkening in body folds (acanthosis nigricans) is a sign of insulin resistance.
Mental Health
PCOS significantly increases the risk of anxiety and depression. The hormonal fluctuations, physical symptoms, fertility concerns, and metabolic disruption all contribute to psychological burden. This relationship is bidirectional — stress and emotional distress worsen hormonal imbalance, which worsens mental health symptoms, creating a loop that is difficult to break without addressing both dimensions simultaneously.
For a full exploration of how PCOS affects mental health, see: Emotional Symptoms of PCOS You Shouldn’t Ignore.
Common Symptoms of PCOS
Symptoms vary considerably in severity and presentation from person to person, which is one reason diagnosis is often delayed.
The most commonly reported symptoms include:
- Irregular, infrequent, or absent menstrual cycles
- Excess hair growth on the face, chest, or back (hirsutism)
- Acne, particularly along the jawline and chin
- Hair thinning or loss on the scalp
- Weight gain, especially concentrated around the abdomen
- Difficulty losing weight despite diet and exercise
- Skin darkening in folds of the neck, groin, or under the breasts
- Fatigue and persistent low energy
- Mood swings, anxiety, or depression
- Difficulty conceiving
For a complete list of symptoms including the less commonly discussed ones, see: Signs of Hormonal Imbalance PCOS You Shouldn’t Ignore.
Hidden and Overlooked Symptoms
Many PCOS symptoms are either dismissed as unrelated or normalized as stress or aging. Several deserve more attention than they typically receive.
Brain fog — difficulty concentrating, poor short-term memory, and mental fatigue — is reported by a significant number of women with PCOS but rarely discussed in clinical settings. It is linked to both insulin resistance and chronic inflammation affecting cognitive function.
Sleep disturbances and obstructive sleep apnea are more common in women with PCOS than in the general population, even in those who are not higher weight.
Gut health issues including bloating, irregular digestion, and sensitivity to certain foods are increasingly recognized as connected to the inflammatory component of PCOS.
Pelvic pain outside of the menstrual cycle can occur and is sometimes mistaken for other conditions.
For a deeper look at the symptoms most people overlook, see: The Hidden Symptoms of PCOS No One Talks About.
What Causes PCOS
The exact cause of PCOS is not yet fully understood. It is considered a multifactorial condition — meaning no single trigger causes it, but rather a combination of genetic, environmental, and lifestyle factors.
Genetic Predisposition
PCOS runs in families. Women with a mother or sister who has PCOS are significantly more likely to develop it themselves. Several genes involved in hormone production, insulin signaling, and inflammatory pathways have been linked to PCOS, though no single “PCOS gene” has been identified.
Hormonal Imbalance
Elevated androgens are both a cause and a consequence of PCOS. High androgen levels prevent normal follicle maturation and ovulation, which in turn leads to more androgen production — a self-reinforcing cycle.
Insulin Resistance
For many women, insulin resistance is not just a consequence of PCOS — it is a contributing driver. High insulin levels directly stimulate ovarian androgen production, and the resulting hormonal imbalance worsens insulin resistance further.
For a deep dive into this mechanism, see: Root Cause of PCOS Hormonal Imbalance.
Chronic Inflammation
Low-grade systemic inflammation can activate androgen-producing pathways in the ovaries independently of insulin levels. Diet, gut microbiome health, stress, and environmental exposures all influence the body’s inflammatory state.
Stress and the HPA Axis
Chronic psychological or physical stress activates the HPA (hypothalamic-pituitary-adrenal) axis, elevating cortisol and adrenal androgens. For women with adrenal PCOS, this is the primary driver of the condition.
For a full explanation of the stress-PCOS connection, see: Can Stress Cause PCOS.
Early Life and Developmental Factors
Emerging research suggests that early-life exposures — including prenatal androgen exposure, childhood trauma, and early-onset puberty — may predispose girls to developing PCOS later in life. This is an area of active research that is reshaping how clinicians think about PCOS prevention.
How PCOS Is Diagnosed
There is no single test that confirms PCOS. Diagnosis is made through a combination of criteria, clinical evaluation, and investigations to rule out other conditions.
Rotterdam Criteria
The most widely used diagnostic framework is the Rotterdam Criteria, which requires at least two of the following three features to be present:
- Irregular or absent ovulation, typically reflected in irregular periods
- Clinical or biochemical signs of elevated androgens (acne, hirsutism, hair loss, or elevated testosterone on blood test)
- Polycystic ovaries on pelvic ultrasound
Meeting two out of three is sufficient for diagnosis — you do not need all three.
Blood Tests
A comprehensive hormone panel typically includes testosterone and DHEA-S (androgen levels), LH and FSH ratio, fasting insulin and glucose, thyroid function, prolactin levels, and sometimes AMH (anti-Müllerian hormone), which correlates with follicle count.
Pelvic Ultrasound
A transvaginal or abdominal ultrasound examines the ovaries for the presence of multiple small follicles and any increase in ovarian volume. The current threshold used in many guidelines is twelve or more follicles per ovary, or an ovarian volume greater than ten milliliters.
Ruling Out Other Conditions
Because PCOS shares symptoms with several other conditions, diagnosis also involves ruling out thyroid disorders, hyperprolactinemia (elevated prolactin), congenital adrenal hyperplasia, Cushing’s syndrome, and other causes of androgen excess.
For a complete guide on what to expect when getting tested, see: How Is PCOS Diagnosed.
PCOS and Mental Health
The psychological burden of PCOS is consistently underestimated in clinical settings. Research shows that women with PCOS are significantly more likely to experience anxiety, depression, and disordered eating compared to women without the condition.
This is not simply a reaction to dealing with a chronic condition. The hormonal imbalances themselves — particularly elevated androgens and cortisol — directly influence mood regulation and stress response. Insulin resistance affects energy levels and cognitive function. The physical symptoms (acne, hair changes, weight fluctuations) carry significant emotional weight and impact body image and self-esteem.
The relationship is bidirectional. PCOS worsens mental health, and poor mental health worsens PCOS. Breaking this cycle often requires addressing both dimensions — not treating the hormonal issues in isolation from the emotional ones.
If you are experiencing persistent anxiety or low mood alongside PCOS symptoms, this deserves attention as part of your overall care plan, not as a separate issue.
For more on this topic, see: Emotional Symptoms of PCOS You Shouldn’t Ignore and Can Stress Cause PCOS.
PCOS and Diet and Nutrition
Diet is one of the most powerful levers available for managing PCOS — particularly for women with insulin-resistant and inflammatory types. What you eat directly affects insulin levels, androgen production, and the inflammatory environment that drives symptoms.
Principles of a PCOS-Supportive Diet
The core dietary approach for PCOS focuses on stabilizing blood sugar, reducing chronic inflammation, and supporting hormonal balance. This generally means prioritizing whole, fiber-rich foods, adequate protein at each meal, healthy fats, and minimizing refined carbohydrates and ultra-processed foods.
The Mediterranean diet and its anti-inflammatory variants have the strongest evidence base for PCOS management. They have been shown to improve insulin sensitivity, reduce androgen levels, and support more regular ovulation.
Foods That Tend to Worsen PCOS
Refined carbohydrates and sugars cause rapid blood glucose spikes that drive insulin surges and androgen production. Dairy and certain saturated fats may worsen inflammation in some women. Highly processed foods contribute to inflammatory load and gut dysbiosis.
Supplements With Evidence
Several supplements have meaningful research behind them for PCOS:
- Myo-inositol and D-chiro-inositol improve insulin sensitivity and have been shown in clinical trials to support more regular ovulation
- Magnesium supports insulin function and reduces cortisol
- Zinc reduces androgen levels and supports skin health
- Spearmint tea has demonstrated androgen-lowering effects in clinical studies
- Omega-3 fatty acids reduce inflammation and support cardiovascular health
For a detailed PCOS meal plan and food guide, see: Best Diet for PCOS Weight Loss and Foods to Avoid With PCOS.
PCOS and Fertility
PCOS is one of the leading causes of anovulatory infertility — infertility caused by irregular or absent ovulation. However, a diagnosis of PCOS does not mean you cannot conceive. The majority of women with PCOS who seek fertility treatment are successful.
Natural Conception
For women with PCOS who are trying to conceive, the first approach is typically lifestyle-based. Even modest weight loss in women with insulin-resistant PCOS can restore more regular ovulation. Dietary changes that improve insulin sensitivity, stress reduction, and addressing nutritional deficiencies all support reproductive function.
Tracking ovulation in PCOS is more complex than for women with regular cycles, as standard ovulation predictor kits can give false positives due to elevated LH levels. Basal body temperature charting and monitoring cervical mucus are often more reliable approaches.
Medical Interventions
When lifestyle approaches are insufficient, several medications are used to stimulate ovulation:
- Letrozole (an aromatase inhibitor) is now considered the first-line medication for ovulation induction in PCOS
- Clomiphene citrate has been used for decades and remains effective for many women
- Metformin can support ovulation by improving insulin sensitivity
- In cases where these options do not work, IVF is an option with generally good success rates in women with PCOS
PCOS During Pregnancy
Women with PCOS have a higher risk of gestational diabetes, preeclampsia, and preterm birth. These risks are manageable with appropriate monitoring and care but make it important to inform your obstetric team of your PCOS diagnosis from the outset of pregnancy.
For a dedicated guide on conception with PCOS, see: Can You Get Pregnant With PCOS.
Treatment Options for PCOS
There is no cure for PCOS, but the condition is highly manageable. The most effective approach combines lifestyle changes with targeted medical support, tailored to your specific type and symptoms.
Lifestyle as First-Line Treatment
For most women, lifestyle changes are the most impactful and sustainable intervention:
- A whole-food, lower-glycemic diet that stabilizes blood sugar and reduces inflammation
- Regular exercise — a combination of resistance training (which improves insulin sensitivity) and moderate aerobic activity
- Prioritizing sleep — poor sleep elevates cortisol and worsens both insulin resistance and androgen levels
- Stress management — particularly important for adrenal PCOS, but beneficial across all types
Medications
- Hormonal birth control regulates menstrual cycles and reduces androgen-related symptoms such as acne and excess hair growth
- Metformin improves insulin sensitivity, supports more regular ovulation, and reduces androgen levels
- Anti-androgens such as spironolactone reduce hirsutism and acne by blocking androgen receptors
- Letrozole or clomiphene are used for ovulation induction in women trying to conceive
- Inositol supplements (myo-inositol in particular) are increasingly used as a gentler alternative to metformin for insulin sensitization
Natural and Complementary Approaches
- Spearmint tea — two cups per day has been shown in clinical trials to reduce free testosterone
- Cinnamon — some evidence for improving insulin sensitivity
- Acupuncture — limited but emerging evidence for supporting more regular ovulation
- Gut health support — emerging research links gut microbiome health to PCOS severity
The right treatment combination depends on your type of PCOS, your primary symptoms, and whether fertility is a current goal. A collaborative approach with a gynaecologist or endocrinologist who understands PCOS is always the most effective path.
Long-Term Health Risks of PCOS
Left unmanaged, PCOS increases the risk of several serious long-term health conditions. Awareness of these risks is not meant to cause alarm — it is meant to motivate proactive management.
Type 2 Diabetes
The chronic insulin resistance at the heart of most PCOS cases significantly elevates the risk of developing type 2 diabetes. Regular blood sugar monitoring and lifestyle management are the primary tools for reducing this risk.
Cardiovascular Disease
PCOS is associated with an unfavorable cardiovascular risk profile — including elevated LDL cholesterol, reduced HDL cholesterol, higher blood pressure, and increased systemic inflammation. These factors combine to raise the long-term risk of heart disease and stroke, particularly after menopause.
Endometrial Health
When ovulation does not occur regularly, the uterine lining (endometrium) is not shed as it should be. Prolonged buildup of the endometrial lining increases the risk of endometrial hyperplasia and, over time, endometrial cancer. This is one of the reasons that regulating menstrual cycles — even if fertility is not a concern — is an important part of PCOS management.
Sleep Apnea
Obstructive sleep apnea is significantly more common in women with PCOS than in the general population, even after controlling for weight. This is thought to be linked to the effects of androgens on upper airway anatomy and respiratory control. If you experience persistent fatigue despite adequate sleep, snoring, or waking feeling unrefreshed, this is worth discussing with your doctor.
Metabolic Syndrome
Women with PCOS are at elevated risk of developing metabolic syndrome — a cluster of conditions including central obesity, high blood pressure, high blood sugar, and abnormal cholesterol levels that together significantly increase cardiovascular risk.
Polycystic Ovaries and Pregnancy
Having polycystic ovaries pregnancy is possible but can be more challenging due to irregular ovulation or hormonal imbalance. Many women with PCOS still conceive naturally or with the help of fertility treatments. Early diagnosis and treatment improve the chances of a healthy pregnancy.
Tip: Always consult a gynecologist or fertility specialist for personalized care.
Can You Get Pregnant with PCOS?
Yes, you can get pregnant with PCOS. While it may take more time or support, many people with PCOS go on to have healthy pregnancies. The key is understanding what might be affecting fertility and choosing the right approach to manage it.
Ovulation Issues
PCOS often affects ovulation due to hormonal imbalances. The ovaries may not release an egg regularly, which can lead to irregular or missed periods. Without consistent ovulation, it becomes harder to predict fertile windows and conceive naturally. However, ovulation is not always completely absent—it may just be irregular, which means pregnancy is still possible.
Treatment Options
There are several ways to improve fertility with PCOS, depending on individual needs.
- Lifestyle changes such as maintaining a healthy weight, balanced diet, and regular exercise can help regulate ovulation
- Medications may be prescribed to stimulate ovulation or improve insulin sensitivity
- In some cases, fertility treatments like assisted reproductive techniques may be recommended
The right treatment plan can significantly increase the chances of conception.
Living Well With PCOS
PCOS is a long-term condition, not a temporary one. The goal is not to cure it but to manage it effectively enough that it no longer dominates your health or quality of life.
The women who manage PCOS most successfully tend to share a few consistent approaches. They treat food as medicine — not in a restrictive or punishing way, but by consistently choosing foods that support hormonal balance. They move their bodies regularly in ways that improve insulin sensitivity without further stressing the HPA axis. Also they take mental health seriously as part of the condition, not separately from it. And they work with clinicians who understand that PCOS is not a single condition with a single solution.
Perhaps most importantly, they give themselves time. PCOS does not respond to interventions overnight. Hormonal systems change slowly. The progress that comes from consistent lifestyle changes over three to six months is real and meaningful — but it requires patience that our instant-results culture makes difficult.
You are not broken. Your body is responding to signals that have become dysregulated. With the right information and the right support, those signals can be rebalanced.
What to Read Next
This guide is the foundation of the PCOS content on this site. Each link below goes deeper on a specific aspect of the condition:
Understanding PCOS
Symptoms
Causes and Triggers
Diet and Management
- Best Diet for PCOS Weight Loss
- Foods to Avoid With PCOS
- Best Supplements for PCOS
- Best Workout Routine for PCOS
Fertility
- Can You Get Pregnant With PCOS
- How to Track Ovulation With PCOS
Treatment
- Metformin for PCOS — What to Expect
- Spearmint Tea for PCOS — Does It Work
Frequently Asked Questions
Can PCOS go away on its own?
PCOS does not resolve entirely on its own, but symptoms can improve significantly — sometimes dramatically — with consistent lifestyle changes. Some women experience a natural reduction in symptoms after menopause, though the underlying hormonal and metabolic factors remain.
Can you have PCOS with regular periods?
Yes. Regular periods do not rule out PCOS. Some women have regular cycles but still have elevated androgens and polycystic ovaries on ultrasound. This is why diagnosis requires meeting the Rotterdam Criteria rather than relying on any single symptom.
Does PCOS always cause weight gain?
No. While weight gain is common in insulin-resistant PCOS, lean PCOS (sometimes called non-heavier person PCOS) affects women of normal or low body weight. The hormonal and metabolic disruptions are present regardless of weight.
Is PCOS genetic?
There is a significant genetic component. Having a first-degree female relative with PCOS roughly doubles your risk. However, genetics is not destiny — lifestyle and environmental factors influence whether and how severely PCOS expresses.
What is the best diet for PCOS?
There is no single universally best diet. The most evidence-backed approaches are anti-inflammatory and lower-glycemic — prioritizing whole grains, vegetables, quality protein, and healthy fats while minimizing refined sugars and highly processed foods. The Mediterranean diet has the strongest research support.
Can teenagers have PCOS?
Yes. PCOS can develop in adolescence, often around the time of puberty. Diagnosing PCOS in teenagers requires extra caution because irregular periods and some acne are normal during early puberty. A diagnosis in adolescents typically requires persistent symptoms over at least two years.
This guide is reviewed and updated regularly. Last updated June 2026. This content is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.